
by Peter A. McCullough, MD, MPH, Ronan J. Kelly, MD, Gaetano Ruocco, MD, Gaetano Ruocco, MD, Edgar Lerma, MD, James Tumlin, MD, Kevin R. Wheelan, MD, Nevin Katz, MD, Norman E. Lepor, MD, Kris Vijay, MD, Harvey Carter, MD, Bhupinder Singh, MD, Sean P. McCullough, BS, Brijesh K. Bhambi, MD, Alberto Palazzuoli, MD, PhD, Gaetano M. De Ferrari, MD, PhD, Gregory P. Milligan, MD, MPH, Taimur Safder, MD, MPH, Kristen M. Tecson, PhD, Dee Dee Wang, MD, John E. McKinnon, MD, William W. O’Neill, MD, Marcus Zervos, MD, Harvey A. Risch, MD, PhD,
The pandemic of severe acute respiratory syndrome coronavius-2 (SARS-CoV-2 [COVID-19]) is rapidly expanding across the world with each country and region developing distinct epidemiologic patterns in terms of frequency, hospitalization, and death. There has been considerable focus on 2 major areas of response to the pandemic: containment of the spread of infection and reducing inpatient mortality. These efforts, although well-justified, have not addressed the ambulatory patient with COVID-19 who is at risk for hospitalization and death. The current epidemiology of rising COVID-19 hospitalizations serves as a strong impetus for an attempt at treatment in the days or weeks before a hospitalization occurs.
Most patients who arrive to the hospital by emergency medical services with COVID-19 do not initially require forms of advanced medical care.
Once hospitalized, approximately 25% require mechanical ventilation, advanced circulatory support, or renal replacement therapy. Hence, it is conceivable that some, if not a majority, of hospitalizations could be avoided with a treat-at-home first approach with appropriate telemedicine monitoring and access to oxygen and therapeutics.
As in all areas of medicine, the large randomized, placebo-controlled, parallel group clinical trial in appropriate patients at risk with meaningful outcomes is the theoretical gold standard for recommending therapy. These standards are not sufficiently rapid or responsive to the COVID-19 pandemic.
One could argue the results of definitive trials were needed at the outset of the pandemic, and certainly are needed now with more than 1 million cases and 500,000 deaths worldwide.
Because COVID-19 is highly communicable, many ambulatory clinics do not care for patients in face-to-face visits, and these patients are commonly declined by pharmacies, laboratories, and imaging centers. On May 14, 2020, after about 1 million cases and 90,000 deaths in the United States had already occurred, the National Institutes of Health (NIH) announced it was launching an outpatient trial of hydroxychloroquine (HCQ) and azithromycin in the treatment of COVID-19.
A month later, the agency announced it was closing the trial because of the lack of enrollment with only 20 of 2000 patients recruited.
No safety concerns were associated with the trial. This effort serves as the best current working example of the lack of feasibility of outpatient trials for COVID-19. It is also a strong signal that future ambulatory trial results are not imminent or likely to report soon enough to have a significant public health impact on clinical outcomes.
If clinical trials are not feasible or will not deliver timely guidance to clinicians or patients, then other scientific information bearing on medication efficacy and safety needs to be examined. Cited in this article are more than a dozen studies of various designs that have examined a range of existing medications. Thus, in the context of present knowledge, given the severity of the outcomes and the relative availability, cost, and toxicity of the therapy, each physician and patient must make a choice: watchful waiting in self-quarantine or empiric treatment with the aim of reducing hospitalization and death. Because COVID-19 expresses a wide spectrum of illness progressing from asymptomatic to symptomatic infection to fulminant adult respiratory distress syndrome and multiorgan system failure, there is a need to individualize therapy according to what has been learned about the pathophysiology of human SARS-CoV-2 infection.
It is beyond the scope of this article to review every preclinical and retrospective study of proposed COVID-19 therapy. Hence, the agents proposed are those that have appreciable clinical support and are feasible for administration in the ambulatory setting. SARS-CoV-2 as with many infections may be amenable to therapy early in its course but is probably not responsive to the same treatments very late in the hospitalized and terminal stages of illness.
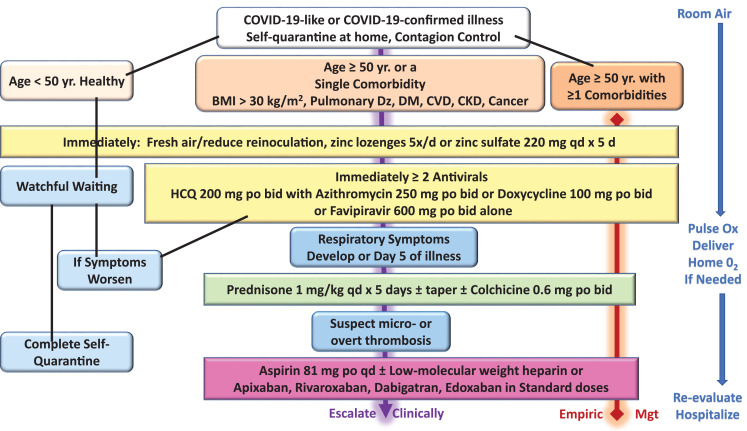
For the ambulatory patient with recognized early signs and symptoms of COVID-19, often with nasal real-time reverse transcription or oral antigen testing pending, the following 4 principles could be deployed in a layered and escalating manner depending on clinical manifestations of COVID-19-like illness
and confirmed infection: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, and 4) antiplatelet/antithrombotic therapy. Because the results of testing could take up to a week to return, treatment can be started before the results are known. For patients with cardinal features of the syndrome (ie, fever, body aches, nasal congestion, loss of taste and smell, etc.) and suspected false-negative testing, treatment can be the same as those with confirmed COVID-19.
Future randomized trials are expected to confirm, reject, refine, and expand these principles. In this article, they are set forth in emergency response to the growing pandemic as shown in Figure 1.

Control of Contagion
A major goal of self-quarantine is the control of contagion.
Many sources of information suggest the main place of viral transmission occurs in the home.
Facial covering for all contacts within the home as well as frequent use of hand sanitizer and hand washing is mandatory. Sterilizing surfaces such as countertops, door handles, phones, and other devices is advised. When possible, other close contacts can move out of the domicile and temporarily stay with others not ill with SARS-CoV-2. Findings from multiple studies indicate that policies concerning control of the spread of SARS-CoV-2 are effective and extension into the home as the most frequent site of viral transfer is paramount.
Reduction of Self-Reinoculation
It is well-recognized that COVID-19 exists outside the human body in a bioaerosol of airborne particles and droplets. Because exhaled air in an infected person is considered to be “loaded” with inoculum, each exhalation and inhalation is effectively reinoculation.
In patients who are hospitalized, negative pressure is applied to the room air largely to reduce spread outside of the room. We propose that fresh air could reduce reinoculation and potentially reduce the severity of illness and possibly reduce household spread during quarantine. This calls for open windows, fans for aeration, or spending long periods of time outdoors away from others with no face covering to disperse and not reinhale the viral bioaerosol.
Combination Antiviral Therapy
Rapid and amplified viral replication is the hallmark of most acute viral infections. By reducing the rate, quantity, or duration of viral replication, the degree of direct viral injury to the respiratory epithelium, vasculature, and organs may be lessened.
Additionally, secondary processes that depend on viral stimulation, including the activation of inflammatory cells, cytokines, and coagulation, could potentially be lessened if viral replication is attenuated. Because no form of readily available medication has been designed specifically to inhibit SARS-CoV-2 replication, 2 or more of the nonspecific agents listed here can be entertained. None of the approaches listed have specific regulatory approved advertising labels for their manufacturers; thus all would be appropriately considered acceptable “off-label” use.
Zinc Lozenges and Zinc Sulfate
Zinc is a known inhibitor of coronavirus replication. Clinical trials of zinc lozenges in the common cold have demonstrated modest reductions in the duration and or severity of symptoms.
By extension, this readily available nontoxic therapy could be deployed at the first signs of COVID-19.
Zinc lozenges can be administered 5 times a day for up to 5 days and extended if needed if symptoms persist. The amount of elemental zinc lozenges is <25% of that in a single 220-mg zinc sulfate daily tablet. This dose of zinc sulfate has been effectively used in combination with antimalarials in early treatment of high-risk outpatients with COVID-19.
Antimalarials
Hydroxychloroquine (HCQ) is an antimalarial/anti-inflammatory drug that impairs endosomal transfer of virions within human cells. HCQ is also a zinc ionophore that conveys zinc intracellularly to block the SARS-CoV-2 RNA-dependent RNA polymerase, which is the core enzyme of the virus replication.
The currently completed retrospective studies and randomized trials have generally shown these findings: 1) when started late in the hospital course and for short durations of time, antimalarials appear to be ineffective, 2) when started earlier in the hospital course, for progressively longer durations and in outpatients, antimalarials may reduce the progression of disease, prevent hospitalization, and are associated with reduced mortality.
,
,
,
In a retrospective inpatient study of 2541 patients hospitalized with COVID-19, therapy associated with an adjusted reduction in mortality was HCQ alone (hazard ratio [HR] = 0.34, 95% confidence interval [CI] 0.25-0.46, P <0.001) and HCQ with azithromycin (HR = 0.29, 95% CI 0.22-0.40, P <0.001).
HCQ was approved by the US Food and Drug Administration in 1955, has been used by hundreds of millions of people worldwide since then, is sold over the counter in many countries, and has a well-characterized safety profile that should not raise undue alarm.
,
Although asymptomatic QT prolongation is a well-recognized and infrequent (<1%) complication of HCQ, it is possible that in the setting of acute illness symptomatic arrhythmias could develop. Data safety and monitoring boards have not declared safety concerns in any clinical trial published to date. Rare patients with a personal or family history of prolonged QT syndrome and those on additional QT prolonging, contraindicated drugs (eg, dofetilide, sotalol) should be treated with caution and a plan to monitor the QTc in the ambulatory setting. A typical HCQ regimen is 200 mg bid for 5 days and extended to 30 days for continued symptoms. A minimal sufficient dose of HCQ should be used, because in excessive doses the drug can interfere with early immune response to the virus.
Azithromycin
Azithromycin is a commonly used macrolide antibiotic that has antiviral properties mainly attributed to reduced endosomal transfer of virions as well as established anti-inflammatory effects.
It has been commonly used in COVID-19 studies initially based on French reports demonstrating markedly reduced durations of viral shedding, fewer hospitalizations, and reduced mortality combination with HCQ as compared to those untreated.
,
In the large inpatient study (n = 2451) discussed previously, those who received azithromycin alone had an adjusted HR for mortality of 1.05, 95% CI 0.68-1.62, and P = 0.83.
The combination of HCQ and azithromycin has been used as standard of care in other contexts as a standard of care in more than 300,000 older adults with multiple comorbidities.
This agent is well-tolerated and like HCQ can prolong the QTc in <1% of patients. The same safety precautions for HCQ listed previously could be extended to azithromycin with or without HCQ. Azithromycin provides additional coverage of bacterial upper respiratory pathogens that could potentially play a role in concurrent or secondary infection. Thus, this agent can serve as a safety net for patients with COVID-19 against clinical failure of the bacterial component of community-acquired pneumonia.
,
The same safety precautions for HCQ could be extended to azithromycin with or without HCQ. Because both HCQ and azithromycin have small but potentially additive risks of QTc prolongation, patients with known or suspected arrhythmias or taking contraindicated medications or should have more thorough workup (eg, review of baseline electrocardiogram, imaging studies, etc.) before receiving these 2 together. One of many dosing schemes is 250 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection.
Doxycycline
Doxycycline is another common antibiotic with multiple intracellular effects that may reduce viral replication, cellular damage, and expression of inflammatory factors.
,
This drug has no effect on cardiac conduction and has the main caveat of gastrointestinal upset and esophagitis. As with azithromycin, doxycycline has the advantage of offering antibacterial coverage for superimposed bacterial infection in the upper respiratory tract. Doxycycline has a high degree of activity against many common respiratory pathogens including Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, anaerobes such as Bacteroides and anaerobic/microaerophilic streptococci and atypical agents like Legionella, Mycoplasma pneumoniae, and Chlamydia pneumoniae.
One of many dosing schemes is 200 mg po followed by 100 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection. Doxycycline may be useful with HCQ for patients in whom the HCQ-azithromycin combination is not desired.
Favipiravir
Favipiravir, an oral selective inhibitor of RNA-dependent RNA polymerase, is approved for ambulatory use in COVID-19 in Russia, India, and other countries outside of the United States.
It has been previously used for treatment of some life-threatening infections such as Ebola virus, Lassa virus, and rabies. Its therapeutic efficacy has been proven in these diseases.
Like, the antimalarials and antibiotics, favipiravir has no large-scale randomized trials completed at this time, given the short time frame of the pandemic. A dose administration could be 1600 mg po bid on day 1, following by 600 mg po bid for 14 days.
Immunomodulators
The manifestations of COVID-19 that prompt hospitalization and that may well lead to multiorgan system failure are attributed to a cytokine storm. The characteristic profile of a patient acutely ill with COVID-19 includes leukocytosis with a relative neutropenia. These patients have higher serum level of cytokines (ie, TNF-α, IFN-γ, IL-1β, IL-2, IL-4, IL-6, and IL-10) and C-reactive protein than control individuals. Among patients with COVID-19, serum IL-6 and IL-10 levels appear even more elevated in the critically ill.
As with any acute inflammatory state, early treatment with immunomodulators is expected to impart greater benefit. In COVID-19, some of the first respiratory findings are nasal congestion, cough, and wheezing. These features are due to excess inflammation and cytokine activation. Early use of corticosteroids is a rational intervention for patients with COVID-19 with these features as they would be in acute asthma or reactive airways disease.
,
The RECOVERY trial randomized 6425 hospitalized patients with COVID-19 in a 2:1 ratio to dexamethasone 6 mg po/IV daily for up to 10 days and found dexamethasone reduced mortality (HR = 0.65, 95% CI 0.51-0.82, P <0.001).
One potential dosing scheme for outpatients starting on day 5 or the onset of respiratory symptoms is prednisone 1 mg/kg given daily for 5 days with or without a subsequent taper.
Colchicine
Colchicine is a nonsteroidal antimitotic drug that blocks metaphase by binding to the ends of microtubules to prevent the elongation of the microtubule polymer. This agent has proven useful in gout and idiopathic recurrent pericarditis. The GRECCO-19 randomized open-label trial in 105 hospitalized patients with COVID-19 found that colchicine was associated with a reduction in D-dimer levels and improved clinical outcomes.
The clinical primary end point (2-point change in World Health Organization ordinal scale) occurred in 14.0% in the control group (7 of 50 patients) and 1.8% in the colchicine group (1 of 55 patients) (odds ratio, 0.11; 95% CI, 0.01-0.96; P = 0.02).
Because the short-term safety profile is well understood, it is reasonable to consider this agent along with corticosteroids in an attempt to reduce the effects of cytokine storm. A dosing scheme of 1.2 mg po, followed by 0.6 mg po bid for 3 weeks can be considered.
Antiplatelet Agents and Antithrombotics
Multiple studies have described increased rates of pathological macro- and micro-thrombosis.
,
Patients with COVID-19 have described chest heaviness associated with desaturation that suggests the possibility of pulmonary thrombosis.
Multiple reports have described elevated D-dimer levels in acutely ill patients with COVID-19, which has been consistently associated with increased risk of deep venous thrombosis and pulmonary embolism.
,
,
Necropsy studies have described pulmonary microthrombosis in COVID-19.
These observations support the notion that endothelial injury and thrombosis play a role oxygen desaturation, a cardinal reason for hospitalization and supportive care.
Based on this pathophysiologic rationale, aspirin 81 mg daily can be administered as an initial antiplatelet and anti-inflammatory agent.
,
Ambulatory patients can be additionally treated with subcutaneous low-molecular-weight heparin or with short-acting novel anticoagulant drugs in dosing schemes similar to those use in outpatient thromboprophylaxis. In a retrospective study of 2773 inpatients with COVID-19, 28% received anticoagulant therapy within 2 days of admission, and despite being used in more severe cases, anticoagulant administration was associated with a reduction in mortality (HR = 0.86 per day of therapy, 95% CI: 0.82-0.89; P <0.001). Additional supportive data on the use anticoagulants reducing mortality has been reported in hospitalized patients with elevated D-dimer levels and higher comorbidity scores.
Many acutely ill outpatients also have general indications for venous thromboembolism prophylaxis applicable to COVID-19.
Delivery of Oxygen and Monitoring
Because ambulatory centers and clinics have been reticent to have face-to-face visits with patients with COVID-19, telemedicine is a reasonable platform for monitoring. Clinical impressions can be gained with audio and video interviews by the physician with the patient. Supplemental information, including vital signs and symptoms, will be important to guide the physician. A significant component of safe outpatient management is maintenance of arterial oxygen saturation on room air or prescribed home oxygen under direct supervision by daily telemedicine with escalation to hospitalization for assisted ventilation if needed. Self-proning could be entertained for confident patients with good at-home monitoring.
Summary



