
By Wolf Moon
Using Principles of Protein Equivalence and Analogy as Predictive Tools for Coronavirus Understanding
Surely you’ve heard of the BROWN RECLUSE SPIDER.

The brown recluse is related to several other recluses, and a couple of other families of spiders, that all have a similar venom – a protein called sphingomyelinase D. This is an enzyme that degrades animal tissues, and is responsible for the very distinctive giant-pock-mark-wound-forming symptoms of recluse bites. The brown recluse does not have as much of this protein in its venom as do some other recluses. The worst recluse, distributed over several countries in South America, has roughly ten times as much sphingomyelinase D as the North American brown recluse. Bites by THAT recluse not only result in deep wounds – they result in SYSTEMIC effects much more often than do bites of the “mere” brown recluse. Fatalities are much more common.
But just stop and think – THAT is how potent protein venoms can be. The tiny bite of a spider with a tiny bit of a protein in it – mere micrograms – can leave a 10-inch hole in the leg, with life-threatening systemic effects.
Snake venoms use different proteins from spiders in their venoms. Some spiders like the black widow have neurotoxic venoms, which affect nervous function, and some snakes like cobras have DIFFERENT neurotoxic venoms.
The honey badger is, weirdly, somewhat immune to the paralyzing neurotoxic cobra venom (jump to near the end of the video).
Many snakes have hemotoxic venoms, and THOSE venoms tend to cause cardiovascular problems. Interestingly, one of those problems is a somewhat rare clotting disorder called thrombocytopenia.
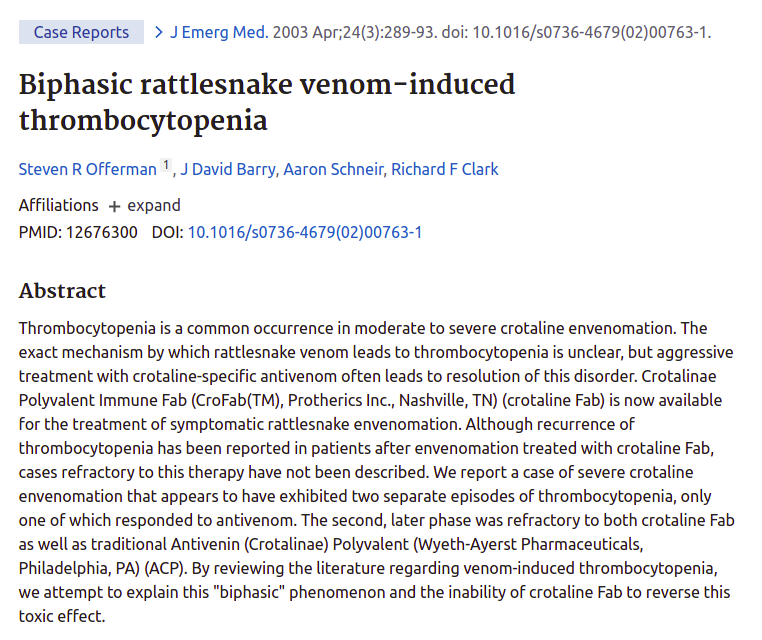
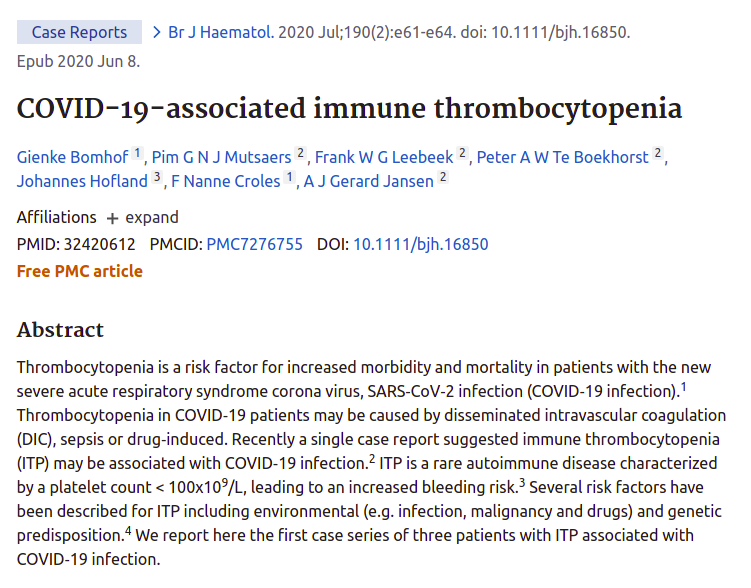
Thus, when I heard that this uncommon symptom was sometimes occurring as a coronavirus vaccine adverse effect, I suspected that there might be a protein cause – the spike protein – acting similarly to proteins in those hemotoxic snake venoms.
If that were the case, we should expect the same effect to be caused by COVID-19 itself, sometimes.
Should we just jump on such an analogy? One that is based on the ASSUMPTION that the spike protein is causing thrombocytopenia? Or at least similarly involved in the two cases?
Let’s think about this.
One of the things which is most fascinating about the BRANCH COVIDIANS – including the high clergy in government and media – is just how STRONGLY they tend to discourage alternative perspectives on COVID-19 – doing so in a way which is alarming even by the normal standards of narrative-setting and enforcement.
For example, at the very beginning, social media gatekeepers were needlessly hostile to Dr. Cameron Kyle-Sidell’s “high-altitude sickness” perspective on COVID-19 hypoxia, despite the fact that this led to a very beneficial new policy on keeping patients OFF vents, probably saving millions of lives, as well as giving us all a better understanding of HOW COVID-19 is and (more importantly) is NOT damaging lungs of patients.
Millions of lives. Think about it. Not a bad save – unless you want a guy named Trump GONE by any means necessary.
Now, some of these “different” perspectives can and do lead to non-working or just plain wrong theories at a micro-level, but so can ANY perspective. Dr. Kyle-Sidell’s ideas led to a variety of hemoglobin-related and malaria-related theories of COVID-19 which were neither fundamentally true nor useful, and which theories died on their own, without any need for censorship, but which were part of a questioning movement which also led to increased recognition of the endothelial nature of the coronavirus attack on patients’ lungs and other organs.
A CHANGE in perspective which WAS and IS fruitful.
Whether we are talking about damage to capillaries in the lungs, vein occlusions in the retina, or organ damage, particularly in the heart or kidneys, it appears that the cardiovascular endothelium is where COVID-19 does the most damage.
Comorbidities which already involve damage or potential damage to blood vessels – particularly diabetes and endocrine or cardiovascular diseases – are thus particularly dangerous, as SARS-CoV-2 and (presumably) its spike protein – which is what attacks cells – would be attacking an already weak point of failure.
LINK: https://www.consumerreports.org/diabetes/why-diabetes-plus-covid-19-is-so-dangerous/
Now – let’s think carefully about IMMUNITY from both DISEASE and VACCINE. BOTH of them are mediated by immunological reaction to the SPIKE PROTEIN.
What should that tell us about VACCINE RISKS?
LINK: https://www.zdnet.com/article/prominent-security-expert-dan-kaminsky-passes-away-at-42/


I want to thank GrandmaInTexas for those two most recent examples of COVID vaccinations precipitating fatal outcomes in people with both diagnosed and undiagnosed comorbidities. For the record, Dan Kaminsky’s vaccine was undoubtedly either Pfizer, Moderna, or Johnson+Johnson, while Actor Vivekh’s vaccine was Covaxin. The former 3 are all genetic vaccines – the latter is inactivated whole virus. All of them use the WHOLE spike protein in some form or another to trigger immunity.
Here is a handy principle which I call “spike protein equivalence”, as a special case of “vaccine immunological equivalence”.
If some affliction, condition, or mere FACTOR happens to be BAD for a potential victim of COVID-19 itself, then it’s also going to be bad for recipients of the vaccine. The difference is only that – most likely – in MOST cases – the vaccine constitutes a far lighter assault on the patient, than the disease itself.
THAT is the basic logic of vaccination. REDUCE THE RISK. But nonetheless, ACCEPT A RISK.
Do not kid yourself. The WHOLE POINT of vaccines is to entertain a lesser risk – a risk that is not as bad as the disease. The only question is “how less bad” does any particular vaccine happen to be. Based upon that information, one has INFORMED CONSENT.
People need to understand risks clearly in order to take those risks smartly.
Or NOT take them. Where the lyric “If you choose not to decide, you still have made a choice” operates against the circling helicopters of COVID-19 and any successor viruses.
When we do not honestly face the risks and benefits of vaccines, we end up with the psychotic disconnect we now see, where people who SHOULD be voices of reason and trust – like the CDC – are LYING and losing half or more of the nation as trusting followers.
Rather than re-hash here how the CDC has lied to us already, or why the handy principles of “spike protein equivalence” and “snake protein analogy” work so well in understanding COVID disease and vaccine risks, let me give you links to my most recent discussions of the relevant thought.
The FIRST ONE is probably the most comprehensive, and helps to understand the rest.
Branch Covidians – Seven Ways To See Through The Phony Pharmageddon of COVID-19
PREFACE I thought that I might withhold this post on Easter Sunday, and then I changed my mind, thanks to Deplorable Patriot, Trump, Gab and Jesus. If anybody ever FOUGHT on Easter Sunday, it was Christ. It’s time to FOLLOW POINT. The Branch Covidians have taken a toll, but the WAR is turning, and – …
Wolf’s Red-Hot Date With Retrotranscriptive Faucipox
Alternate Title: Is Persistent Reverse Transcription a Hidden Virus/Vaccine Objective? Gloating Pre-Preface There are few feelings of satisfaction like opening up the NEWS and knowing one’s theories and understandings are WORKING even better than one thought. Let’s see if they use this one for damage control, and get the “new science” out before the STORY …
Johnson+Johnson Vaccine Follows Pfizer, Moderna, and AstraZeneca into Problem Territory, and Proves Once Again – Clinical Trials Have Limits
Every coronavirus vaccine so far has shown us SOME defect upon mass release, which was NOT evident in EVEN phase III clinical trials. Look HERE for a searchable PDF document of adverse effects from the Pfizer vaccine: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977005/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf Check out these videos on the low-platelet clotting problem from the Oxford/AstraZeneca vaccine. Here is a fantastic …
Are Clotting Problems a General Minor Risk of COVID Vaccines?
I saw an excellent explanation of the clotting problem with the AstraZeneca vaccine against SARS-CoV-2 / COVID-19 here: The doctor, Dr. ZDogg, MD, offers an exceptionally clear explanation of both what is going on with the AstraZeneca vaccine, and why its distribution was halted or limited in some places for some age groups of patients. …
I am not the only person who is seeing that the SPIKE PROTEIN and variants are interesting beasts. Cthulhu tipped me off to THESE TWO GEMS by Karl Denninger, which are extraordinarily worthwhile:
No Doctor, You’re Wrong
I Hate Being Right
Even though these deal primarily with spike protein equivalence rather than the snake protein analogy, the latter of which Cthulhu mentioned in his tip (he knew I would like these), there is some even more shocking perspective in the second link, in which Denninger simply asks – why did we use the WHOLE sequence of the spike protein which we received from China?
Beyond simple blame games, in which I could postulate that “whole spike protein vaccines” may have resulted from dumb psychology, or even malicious treachery by one or more parties, I can ALSO place Denninger’s question in the context of both failing to ask “Stoecker questions” about “should we base vaccines on the WHOLE spike protein?”, AND the idea that – intentionally or unintentionally – by whoever – we essentially fell into China’s version of the plot of Species…..
Is such “gain of function” good or bad? One could view horsepox-based smallpox vaccine adoption as “gain of function” – a low-level example of the intelligent acceleration of evolution as a “natural” part of evolution itself.
As an aside, IMO the reason they use women for these scenes is ultimately the same reason the spike protein seems to target women’s physiology more than men’s, and that men are actually the first utilitarian sex robots, but – well – it’s so simple, it’s complicated. Patriarchy is both overrated and overstated, shall we just say.
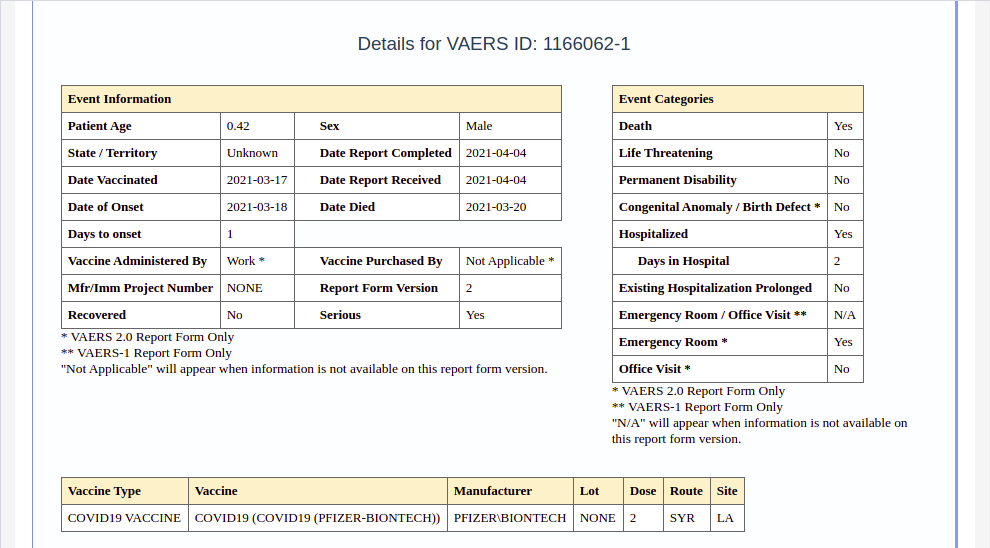
ANYWAY, back to snakebite. “Cleopatra meets spike protein” – only worse.
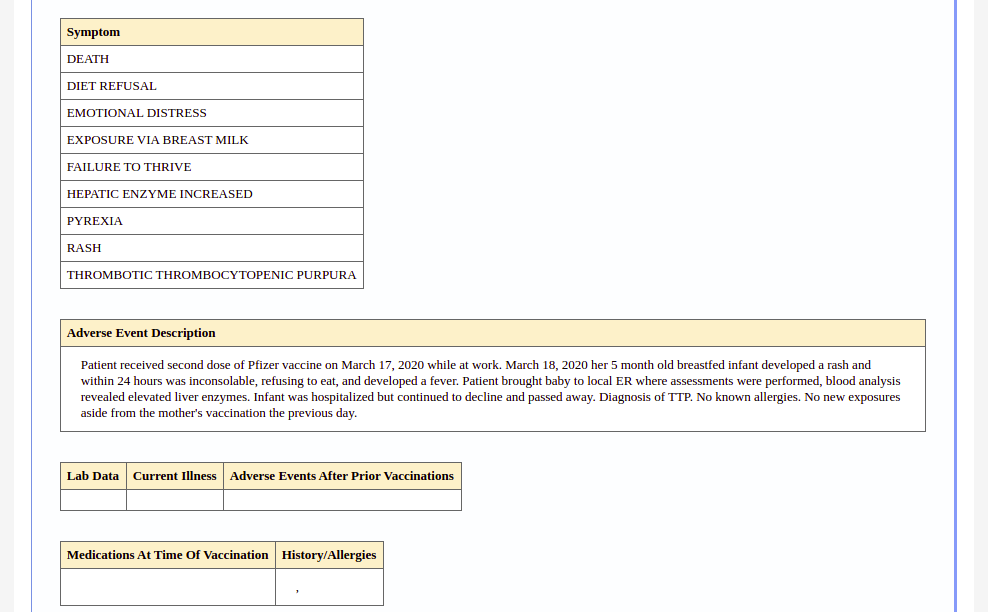
I actually saved that whole report, which is not easily linked, as a series of images:
Before I go on, let me just say that immunology strikes me as a lot like quantum mechanics. If anybody says they truly understand it, it’s almost a sign that they don’t. Nevertheless, basic suspicions work like crazy in either field, which is, again, interesting. In either field, it doesn’t take a genius to see that – 99% of the time – a snake in the grass IS a snake in the grass.
Already, the entire Snopesian Empire is fired up over this case.
LINK: https://www.snopes.com/fact-check/breastfeeding-baby-covid-vaccine/
SEEK anything related, and you will FIND – both WHEAT and CHAFF.
READ, and you will FIND – both INTERESTING and HOLLOW.
No matter how many guns they get working and belt-fed, cross-firing with their diversionary strawman arguments on this one case, the fact of the matter is that TTP is intimately linked to immune disorders, immune responses, and vaccination, so if it shows up, vaccines are and will remain the likeliest suspect NO MATTER WHAT. All Fauci’s horses and all Pfizer’s men are not going to get rid of the NOTABLY MANY cases of TTP , other thrombocytopenic clotting disorders, and clotting disorders in general, which are showing up in (1) COVID cases, (2) COVID recoverees, (3) vaccination adverse events, and (4) vaccination of recoverees in particular.
The relationship of TTP to vaccines and “malappropriate antibodies” in particular is UNDERSTOOD SCIENCE. This is not going away, despite the near-dogmatic narrative that “COVID vaccines do no harm” at the public level, reinforced by the narrative that “fighting vaccine hesitancy is worth LYING about adverse effects”.
No, it’s not.
Skip the following scientific review unless you feel nerdy. I recommend just skimming in either case. But I promise – the deeper you dig here, the more WHEAT you will find.
CLINICAL PLATELET DISORDERS| MAY 25, 2017
Thrombotic thrombocytopenic purpura
Bérangère S. Joly , Paul Coppo , Agnès Veyradier
Blood (2017) 129 (21): 2836–2846.
https://doi.org/10.1182/blood-2016-10-709857
- Abstract
- Introduction
- Historical milestones for TTP understanding
- Definition and pathophysiology
- Diagnosis
- Focus on some specific TTP cases
- Prognosis and follow-up
- Treatment
- Conclusion
- Acknowledgments
- Authorship
- References
Abstract
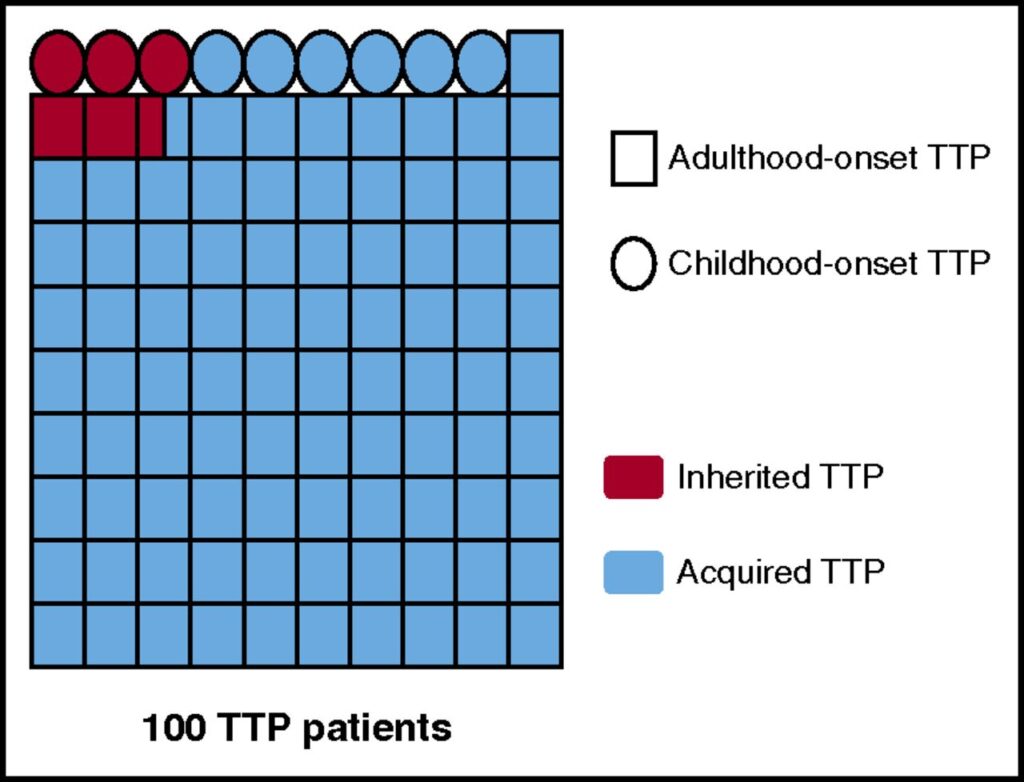
Thrombotic thrombocytopenic purpura (TTP) is a rare and life-threatening thrombotic microangiopathy characterized by microangiopathic hemolytic anemia, severe thrombocytopenia, and organ ischemia linked to disseminated microvascular platelet rich-thrombi. TTP is specifically related to a severe deficiency in ADAMTS13 (a disinterring and metalloprotease with thrombospondin type 1 repeats, member 13), the specific von Willebrand factor-cleaving protease. ADAMTS13 deficiency is most frequently acquired via ADAMTS13 autoantibodies, but rarely, it is inherited via mutations of the ADAMTS13 gene. The first acute episode of TTP usually occurs during adulthood, with a predominant anti-ADAMTS13 autoimmune etiology. In rare cases, however, TTP begins as soon as childhood, with frequent inherited forms. TTP is ∼2-fold more frequent in women, and its outcome is characterized by a relapsing tendency. Rapid recognition of TTP is crucial to initiate appropriate treatment. The first-line therapy for acute TTP is based on daily therapeutic plasma exchange supplying deficient ADAMTS13, with or without steroids. Additional immune modulators targeting ADAMTS13 autoantibodies are mainly based on steroids and the humanized anti-CD20 monoclonal antibody rituximab. In refractory or unresponsive TTP, more intensive therapies including twice-daily plasma exchange; pulses of cyclophosphamide, vincristine, or cyclosporine A; or salvage splenectomy are considered. New drugs including N-acetylcysteine, bortezomib, recombinant ADAMTS13, and caplacizumab show promise in the management of TTP. Also, long-term follow-up of patients with TTP is crucial to identify the occurrence of other autoimmune diseases, to control relapses, and to evaluate psychophysical sequelae. Further development of both patients’ registries worldwide and innovative drugs is still needed to improve TTP management.
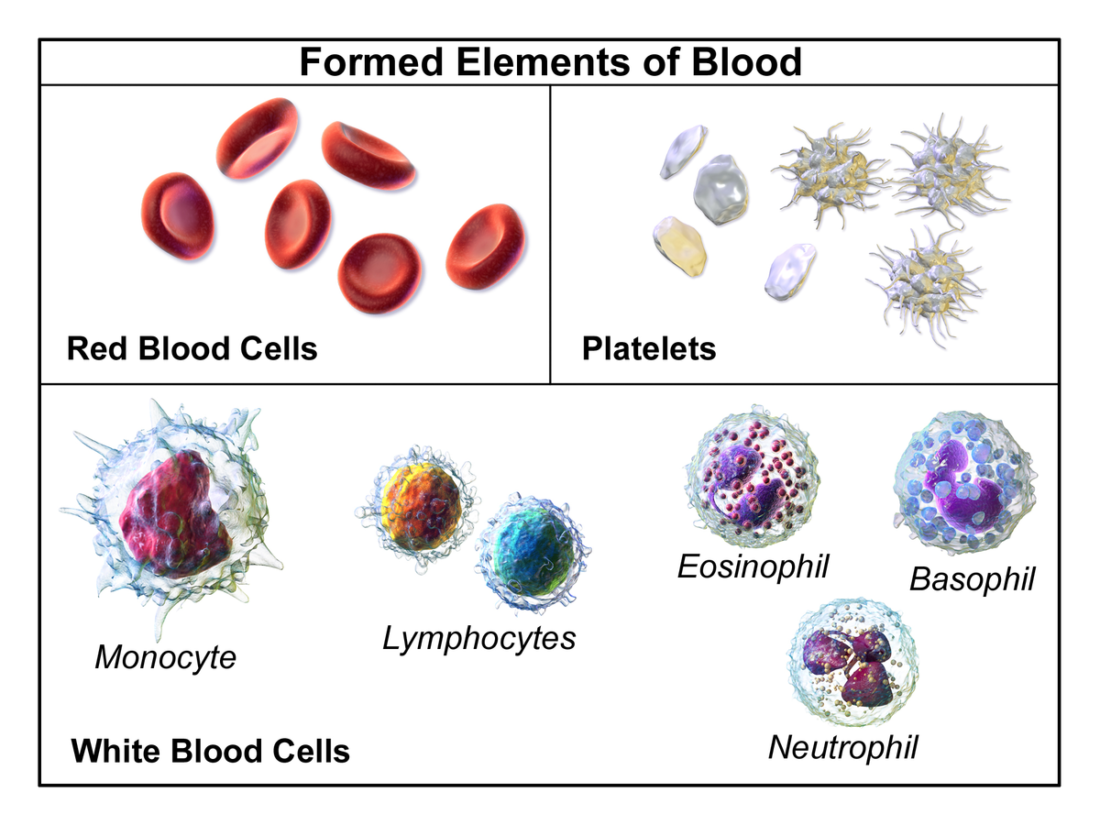
So what does TTP look like?
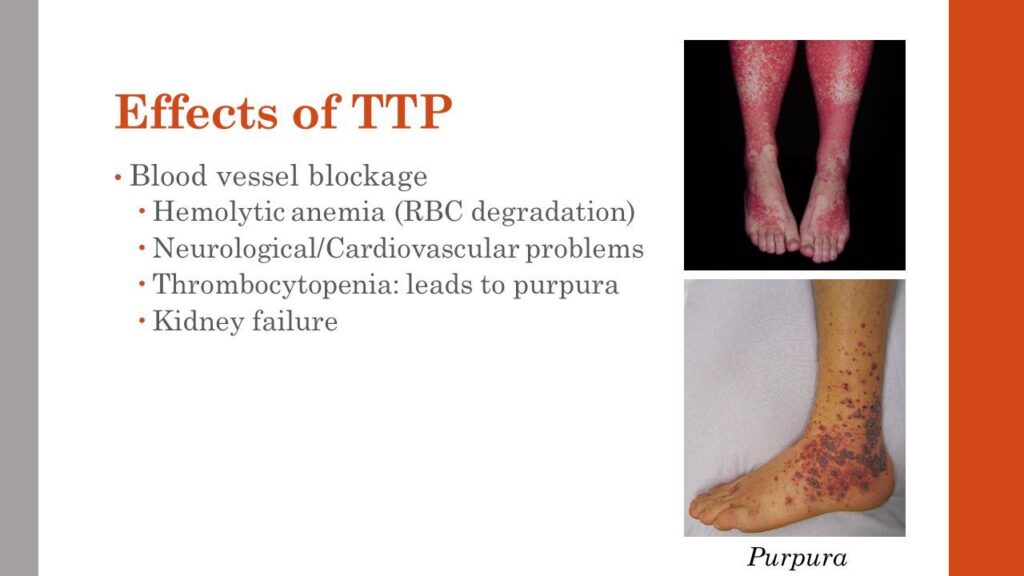
See those pictures? You may want to THINK TWICE about the coronavirus vaccine if you ALREADY have this risky potential outcome of either the disease or the vaccine. I have a link showing that TTP is a high risk in COVID recoverees who get any of the vaccines – I just can’t find it now.
We ARE seeing some public recognition of adverse effects now:
However, as is visible in this article, we are not seeing ANY contraindications to vaccination being admitted publicly. The advice tends to be “get vaccinated, and if you don’t die, but have bad symptoms, see your doctor.
“Sure, Dr. Stalin. Sure. Say – you don’t have any recommendations to PREVENT THIS from happening again to somebody else now, do you? Those would be called ‘contraindications’. Most drugs have them.”
However, I think some recognition is coming. And why is that? Well…..
In my previous post…..
Is The Abortion Vaccine Right For You?
“When the people have any power to object to a socialist solution, a deniable 5% fait accompli is always more desirable to socialists than a negotiated 50% solution, because they can always negotiate on the remaining 95%.” -Wolf Moon When I first heard about a case of a miscarriage by a pregnant doctor, due to …
…..we discussed other disorders – affecting reproductive health, you might say – that MAY or MAY NOT be mediated through the SAME or DIFFERENT activities of the spike protein.
THAT is an interesting question, actually. How economic is spike protein activity? How MUCH strategic information is carried, and at what density? How efficient ARE proteins at carrying smaller-molecular strategies into “genetic warfare”? We may not have those answers yet – and certainly not in PUBLIC SCIENCE – for some time.
Still, I think these questions will eventually be asked and answered, because the menstrual/gestational and clotting effects of the vaccines are so startling, that people are going to ask questions and get answers, whether the “mainstream” (meaning government/corporate) media wants to ask them or not, or to see them answered.
In that regard, we will carry on, asking questions and getting answers, carrying the principle of SPIKE PROTEIN EQUIVALENCE with us, as a handy and useful physiological tool.
The idea of SNAKE PROTEIN ANALOGY will become less of a medical utility, and more of a METAPHOR.

LINK: https://stephenwardeanderson.blogspot.com/2014/11/the-temptation-of-eve.html
There is a refreshing honesty and innocence in this guy’s work. But more than that, he just has a way of catching small details that everybody else misses, and making them beautifully prominent. His portraits of famous figures are quite wonderful in this way. He will completely drop many of the features of those people that I love and see prominently as part of my personal recognition algos, and yet childishly play up awesome things I never noticed.
And with that, let’s talk about Eve.
Our next installment is going to go BACK IN TIME, and show you something very startling about WHEN all this COVID vaccine technology was actually invented.
A lot earlier than anybody wants to admit publicly. Here is a hint.



